MCED and Traditional Screening: A Comprehensive, Complementary Strategy
Traditional cancer screenings such as mammography and colonoscopy remain essential tools that have reduced cancer deaths for decades. Yet, these tests only cover a few cancer types and depend on visible or accessible tissue changes. Multi-Cancer Early Detection (MCED) tests — based on a simple blood draw — do not replace these tests but complement them by finding signals from cancers that currently have no standard screening method. Together, they might create a more comprehensive, layered approach to early detection.
 MCED and Traditional Screening: A Comprehensive, Complementary Strategy
MCED and Traditional Screening: A Comprehensive, Complementary Strategy
Overview of MCED and Traditional Screening
Traditional cancer screenings for breast, lung and colorectal cancers have saved millions of lives through early detection. But what about the other types of cancer that don’t have a screening test? This is where MCED (Multi-Cancer Early Detection) technology might come in, complementing and enhancing your existing screening strategy.
Screening context
Cancer screening recommendations may differ slightly across regions, depending on local healthcare policies, population risk, and national guidelines. Below are the general global and Singapore-specific recommendations based on international and national authorities.
Current screening recommendations in global
- Breast cancer: Biennial mammography for women aged 40 and above (1).
- Colorectal cancer: Begin regular stool-based test or colonoscopy at age 45 (1).
- Lung cancer: Annual low-dose computed tomography (LDCT) for adults aged 50–80 who have a 20 pack-year smoking history and currently smoke or have quit within the past 15 years (1).
- Cervical cancer: Cervical cytology (PAP smear) every 03 years for women aged 21-29; every 03 years with cervical cytology alone, every 05 years with high-risk HPV (hrHPV) testing alone, or every 05 years with hrHPV testing in combination with cytology (cotesting) for women aged 30 to 65 (1).
- Prostate cancer: Prostate–specific antigen (PSA)–based testing starting at age 55 for men (1).
Current screening recommendations in Singapore
- Breast cancer: For women aged 50–69, mammography every 2 years (2).
- Colorectal cancer: In Singapore, men and women aged 50 years and above are eligible for colorectal cancer screening, with a recommended interval of at least 1 year after a previous normal screening result (3).
- Cervical cancer: women aged 25–29 are advised to undergo a Pap smear every 3 years, while those aged 30-69 should have an HPV test every 5 years (4).
Note: Screening guidelines evolve as new evidence emerges. Individuals are encouraged to consult healthcare professionals to determine the most suitable screening schedule for their age and risk profile.
MCED Technology
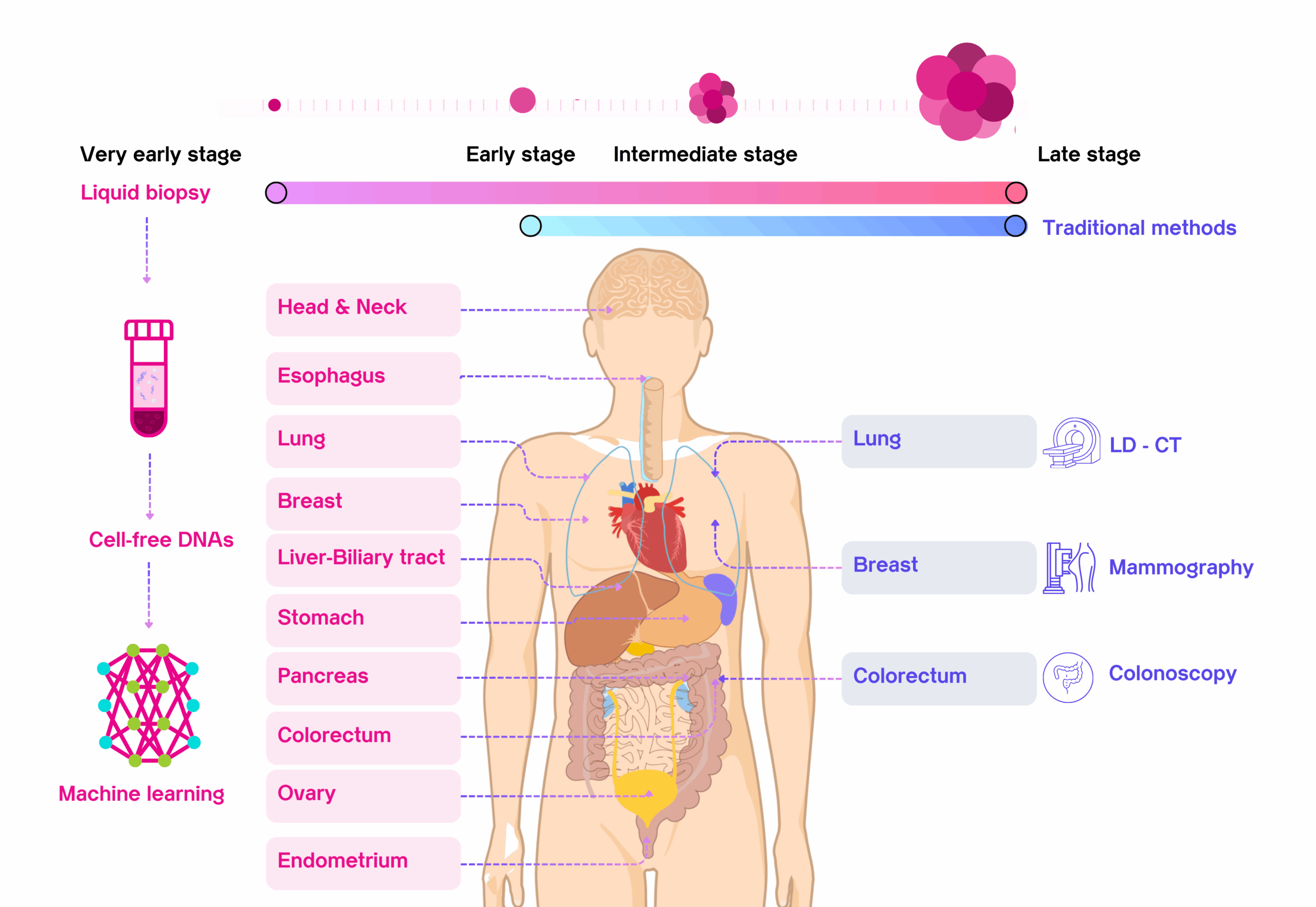
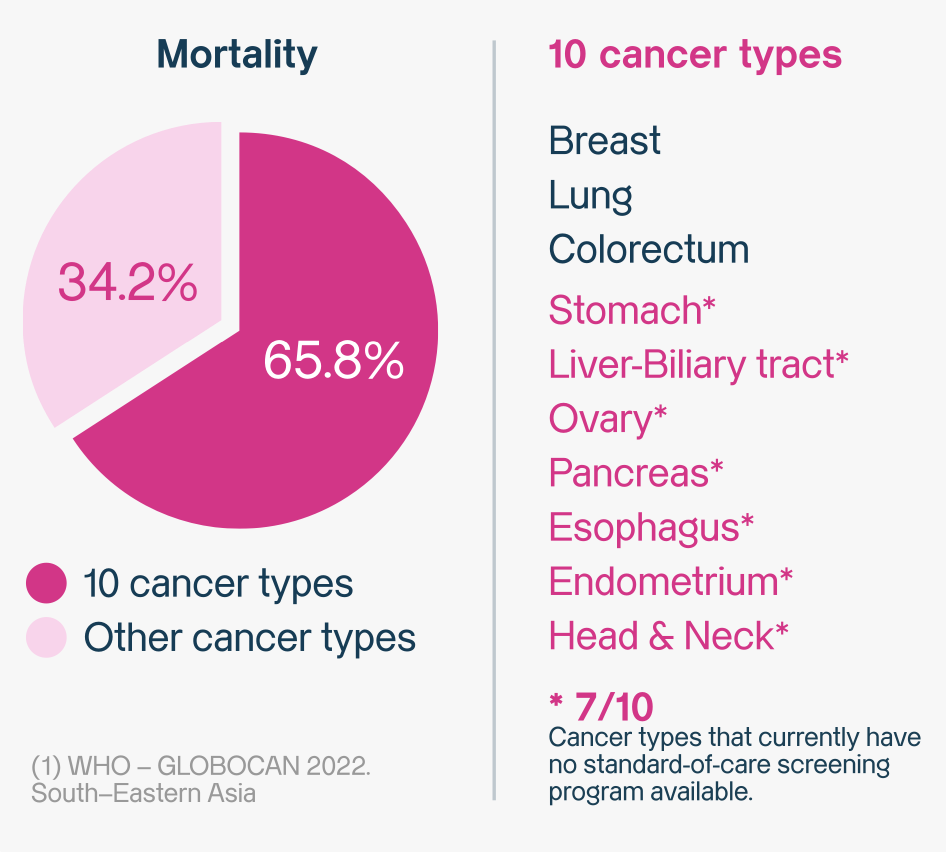
MCED (Multi-Cancer Early Detection) is an emerging technology that may help detect multiple cancers that traditional screenings might miss. In this article, we will focus on MCED applications across the ten most common cancer types, which together account for the majority (65.8%) of cancer mortality worldwide (5).
How does MCED work?
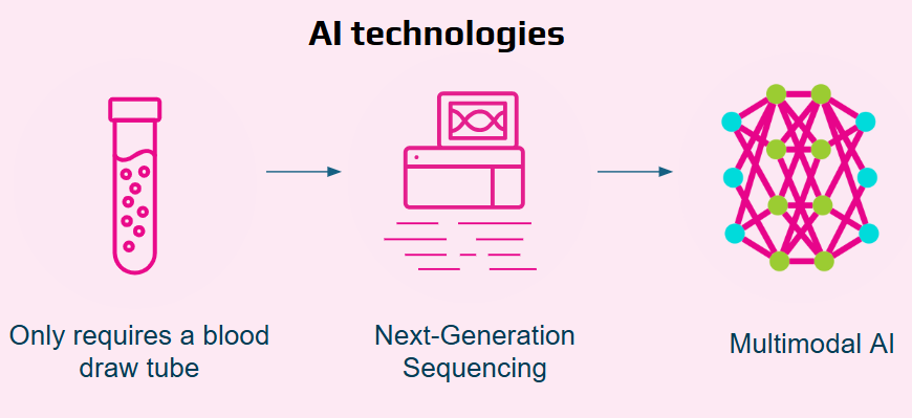
- Detection Method: It’s a simple blood test, sometimes called a “liquid biopsy.” It looks for tiny bits of DNA and other markers that tumors can release into your bloodstream (6).
- Cancer Coverage: A single test can screen for signals from 10 different types of cancer at the same time. This includes many cancers that currently have no other screening method (7).
- Technology Basis: The test applies a multi-omics approach, combining genetics (DNA mutations), epigenetics (methylation signals) and fragmentomics (cfDNA fragmentation patterns) to improve detection accuracy (8).
- Requirement: All it takes is a single blood draw, making the test generally less invasive than other screening procedures.
- Results Timeline: You and your doctor will typically receive the typically 12 working days; timelines may vary by provider, which allows for making a quick decision.
- Clinical Role: MCED tests are designed to be used with, not to replace, current screenings like mammograms. The goal is to create a more complete and powerful strategy for detecting cancer early.
MCED and common screening method
| Aspect | MCED (Multi-Cancer Early Detection) – SPOT-MAS | Traditional Screening |
| Scope of detection | Screens for signals from 10 major cancers and 75 subtypes in one blood test (8). | Focuses on one cancer at a time (e.g., mammogram, colonoscopy). |
| Markers analyzed | ctDNA features interpreted by computational algorithms. | Specific proteins or imaging findings tied to single cancer type |
| Availability | Emerging in clinical practice; adoption varies by region. | Widely established for select cancers (e.g., breast, lung, colorectal). |
| Detection of cancers without standard screening | Yes — includes cancers like liver–biliary tract, stomach, esophagus, ovary, pancreas, endometrium, head & neck. | No — limited to cancers with long-standing screening programs. |
| Patient experience | Minimally invasive — single blood draw. | May involve invasive or uncomfortable procedures. |
| Integration with care | Complements existing methods; supports follow-up diagnostics. | Functions independently for specific cancers. |
MCED is not a replacement for traditional screening. It is designed to work alongside established programs, offering broader coverage and supporting earlier detection where standard protocols may not exist.
Why are both approaches important?
Using both traditional screening and MCED tests together might create a much more powerful strategy for finding cancer early. Think of it like putting together a puzzle: traditional tests give you the essential edge pieces, while MCED tests could help fill in the middle. MCED appears to be particularly useful in detecting cancers that currently have no established screening method. By potentially combining the unique strengths of both approaches, doctors may gain a more complete picture of a patient’s health.
Proof from Clinical Studies:
- Finding Hidden Cancers: In real-world use, MCED tests have successfully detected cancer types which have no standard-of-care screening program available, such as stomach cancer.
Clinical Case: Outsmarting Breast Cancer with Multi-Omics ctDNA
- Pinpointing the Location: Certain MCED tests can accurately predict where a cancer signal is coming from in the body. This is extremely important for guiding doctors on the right next steps for follow-up care.
Benefits of using both methods
When patients and doctors use both traditional screening and new MCED tests, they gain several important benefits:
- Broader cancer coverage: This combined strategy allows you to screen for the common cancers covered by traditional tests, plus the other types that currently have no screening method (7).
- Chance of catching cancer early: Creating more opportunities to find cancer reduces the risk that an early-stage cancer will be missed, providing a stronger safety net for your health.
- Improved patient outcomes: Finding cancer earlier is key. Studies show that MCED tests can help identify cancers at treatable stages, which gives patients a better chance for successful treatment (10).

MCED Technology Introduction
How MCED Complements Traditional Screening
How can both MCED and mammography work better together?
The two tests may work best when used in combination. Mammography remains one of the most effective methods for breast cancer screening while an MCED blood test could help address some of its limitations. The most effective approach may depend on individual health factors and personal risk levels.
For women with dense breasts, mammography can sometimes miss cancers that are masked by dense tissue (12). Adding an MCED test may offer an extra layer of screening, since its accuracy is less likely to be affected by breast density.
In summary, the MCED test is not intended to replace a mammography. Rather, it may serve as a useful complementary tool in situations where a mammography might have limitations—such as in women with dense breasts or in identifying cancers that may arise between scheduled screenings.

MCED and Mammography
MCED and Colonoscopy
Screening for colorectal cancer saves lives, and different methods can complement each other to improve detection. While colonoscopy remains the gold standard for identifying and removing precancerous lesions, the new multi-cancer early detection (MCED) blood test can play a supportive role by detecting molecular signals of cancer that might be missed or develop between screening intervals.
Together, these approaches may offer a more comprehensive view of an individual’s health — combining the preventive power of colonoscopy with the convenience and systemic insight of MCED testing.
What is colonoscopy?
A colonoscopy is widely regarded as the reference standard for polyp detection: it can both find and fix a problem in a single session. It is the screening test that can actually prevent cancer by allowing a doctor to find and remove pre-cancerous growths (called polyps) on the spot.
| Feature | Colonoscopy |
| How it works | A doctor uses a tiny camera to look directly at the inside of your entire colon. |
| How accurate is it? | The specificity of the test is 89% (14), which means that for 1,000 people known not to have colorectal cancer, 890 get a negative result and 110 receive a false-positive. |
| Key advantage | It can prevent cancer. If the doctor finds any pre-cancerous growths (polyps), they can remove them right away during the procedure. |
| What are the downsides? | It is an invasive procedure that requires a full “bowel prep” the day before. In some cases, you will need sedation, and there is a small risk of complications. |
| What is the experience like? | The process involves the bowel preparation diet, sedation for the procedure, and some potential discomfort. |
What makes MCED blood tests special?
An MCED test’s main benefit is its ability to screen for many types of cancer at once with a simple blood draw. It uses advanced technology to find tiny pieces of DNA that tumors release into the bloodstream — called circulating tumor DNA, or ctDNA. In this section, data on MCED performance are referenced from the K-DETEK Study, which evaluated blood-based multi-omics testing for colorectal cancer detection (8).
| Feature | MCED Cancer Detection |
| How it works | The test analyzes ctDNA in the blood using a multi-omics approach, looking for cancer-specific genetic mutations, epigenetic methylation patterns, and fragmentation profiles (fragmentomics) that together form unique cancer signatures. |
| How often is it needed? | It can be used as part of a regular, ongoing screening plan. The recommended time between tests is still being determined (TBD). |
| How accurate is it? | The negative predictive value of the test is 99.9% (8), which means that for every 1000 ASYMPTOMATIC cases with negative results, about 999 cases actually do not have cancer.
The positive predictive value of the test is 39.5% for cancerous lesions and 58.1% when combined with the assessment of precancerous lesions in the digestive tract (8), which means that for every 100 positive test results, 58 patients will actually have cancer or precancerous lesions. Therefore, a positive result should be evaluated by an oncologist, genetic specialist and confirmed by diagnostic imaging tests. |
| What are the biggest benefits? | It’s non-invasive (just a simple blood draw), so no special diet or sedation is needed. A major benefit is that the same test also screens for many other types of cancer. |
| What are the downsides? | Some cancers may not release enough ctDNA into the bloodstream at early stages, so false negatives can occur. |
| What is the experience like? | A blood draw is minimally invasive; individual experience may vary. |
| How easy is it to get? | MCED should be considered and ordered by licensed healthcare professionals; access varies by country and clinic. |
When is MCED typically considered (including for colorectal cancer risk)?
An MCED blood test may be the most appropriate choice in these situations. This screening test is intended for adults aged 45 years and older, particularly those at elevated risk for cancer (15, 16).
- First-degree relative with colorectal cancer or advanced high-risk polyps.
- Personal history of inflammatory bowel disease or cystic fibrosis. Carrying a germline mutation in hereditary cancer syndromes (e.g., Lynch syndrome, polyposis syndrome, etc.).
- Suspected clinical signs (e.g., changes in bowel habits lasting ≥3 weeks WITHOUT response to medication…).
How can both improve outcomes together?
A colonoscopy remains irreplaceable for prevention and polyp removal. However, because colonoscopy is typically performed only every 3–5 years, long intervals can leave room for interval cancers to develop. Additionally, for individuals unwilling or unable to undergo invasive procedures, an MCED test can offer additional monitoring during these gaps — and importantly, it screens for cancers beyond the colon.
When combined thoughtfully, colonoscopy provides prevention through polyp removal, while MCED adds broader detection coverage and supports continuous vigilance between colonoscopies.
If you are eligible for screening, the crucial next step is to consult with your healthcare provider. Together, you can weigh the distinct advantages of each test: the high accuracy and preventative power of a colonoscopy versus the convenience and broader cancer-detecting scope of an MCED blood test.

MCED and Colonoscopy – A Comprehensive, Complementary Strategy
Evaluation of MCED and Traditional Cancer Screening
Cancer screening is evolving rapidly, moving from single-organ tests to multi system screening. Understanding the core detection mechanisms is key to appreciating how different technologies from traditional imaging to new blood tests work together to find cancer earlier.
Imaging-based
This is the most common and established method, relying on structural visualization.
- Mechanism: These tests visualize anatomical changes or tumor masses within the body. They look for lumps, nodules, or density changes characteristic of cancer.
- Application: Imaging excels in established cancer sites (like the breast or lung) and for symptomatic evaluations. Their high resolution provides immediate structural results.
- Limitations: The primary drawback is the size threshold a tumor must be large enough to be seen. These tests are also typically limited to a single organ system per procedure and may involve radiation exposure.
Biomarker-based
MCED represents the future of screening, using molecular signals found in blood.
- Mechanism: This non-invasive approach applies a multi-omics analysis of circulating tumor-derived signals in blood, integrating genetics (mutations), epigenetics (methylation patterns) and fragmentomics (cfDNA fragmentation profiles) to improve early cancer detection.
- Application: MCED is transformative for asymptomatic screening and for detecting inaccessible tumors (like pancreatic or ovarian cancer) for which no other routine screen exists. It offers systemic detection across 10+ cancer types simultaneously.
- Limitations: Some cancers may not release enough ctDNA into the bloodstream at early stages, so false negatives can occur.
Technology integration
No single test is perfect — but each plays a crucial role. Traditional screening methods provide anatomical precision and immediate treatment capability, while MCED offers systemic screening for cancers invisible to conventional scans. Integrating both forms the foundation of a comprehensive, precision-based screening ecosystem. The most effective approach integrates these technologies to maximize detection:
- Complementary Strengths: MCED technology using ctDNA signal can flag cancer in its earliest, asymptomatic phase, while traditional screening methods provide the high resolution confirmation and therapeutic action needed.
- Comprehensive Approach: Using MCED addresses screening gaps by looking beyond single organ systems. A positive biomarker result can risk stratify a patient, informing the frequency and type of follow up imaging required.
How do healthcare professionals decide the suitable approach?
Personal factors
When considering cancer prevention, many people wonder about the benefits of MCED and traditional screening. While methods like mammography or colonoscopy remain essential, Multi-Cancer Early Detection (MCED) tests provide a broader and more convenient option. Beyond clinical effectiveness, patients often choose MCED for personal reasons:
- Peace of mind: Reassurance from checking multiple cancers at once with a single blood draw.
- Comfort & convenience: A quick, non-invasive alternative to procedures like colonoscopy or mammography.
- Broader coverage: Detects cancers not usually covered by standard screening programs.
- Early intervention: Increases chances of simpler treatments and better survival outcomes.
- Personalized awareness: Tailored insight for those with hereditary risks, lifestyle factors, or aging concerns.
Scientific aspects
Advances in medical science are reshaping how cancers are detected at earlier, more treatable stages. The Multi-Cancer Early Detection (MCED) test leverages cutting-edge technology to go beyond the limits of single-cancer screenings. From a scientific perspective, several aspects make MCED testing stand out:
- Liquid biopsy technology: Analyzes circulating tumor DNA (ctDNA) fragments from a simple blood draw.
- Multi-omics approach: Combines genetics, epigenetics, and fragmentomics to enhance detection accuracy.
- AI-driven analysis: Uses advanced machine learning to identify cancer signals and predict tumor origin.
- High specificity and sensitivity: Accurately detects cancers at earlier stages while minimizing diagnostic errors.
- Clinical validation: Supported by large-scale studies with thousands of participants and peer-reviewed evidence.
MCED technology
Frequently Asked Questions
Q: What is the difference between MCED and traditional screening?
A: Traditional screening focuses on detecting one type of cancer at a time (e.g., mammography for breast cancer, colonoscopy for colorectal cancer). MCED (Multi-Cancer Early Detection) uses a simple blood test to detect signals from multiple cancers simultaneously.
Q: Does MCED replace traditional cancer screening tests?
A: No. MCED is designed to complement, not replace, existing methods. Traditional tests remain essential for prevention and early diagnosis of specific cancers, while MCED helps fill gaps by detecting many cancers without established screening protocols.
Q: Can MCED detect cancers that traditional screening misses?
A: Yes. MCED is particularly useful for detecting cancers without established screening methods, such as ovarian and pancreatic cancers, and recent evidence also shows it may help in challenging areas like distinguishing early-stage breast cancer from benign lesions.
Q: Should healthcare providers choose MCED or traditional screening?
A: The approach is a combination. Patients should follow national guidelines for traditional tests and consider MCED as an additional tool for more comprehensive coverage.
Conclusion
The future of cancer screening is not about choosing one test over another — it is about integration. Traditional screening remains the cornerstone of prevention and diagnosis, while MCED extends the reach to cancers that otherwise go unnoticed. Together, they close the gaps in early detection and represent the next generation of precision prevention — early, broad, and personalized.
Disclaimer: This content is for educational purposes only and does not constitute medical advice. Multi-Cancer Early Detection (MCED) tests should be considered and ordered by licensed healthcare professionals. Availability and regulatory permissions vary by country.
Reference:
(1) U.S. Preventive Services Task Force (USPSTF) recommendations
(2) HealthHub. “Evidence-based Recommendations on Health Screening Tests.” HealthHub Singapore (2025). Retrieved October 20, 2025, from https://www.healthhub.sg/well-being-and-lifestyle/personal-care/type-2-screening-tests
(3) Health Promotion Board. Healthier SG Screening: Are you eligible for subsidised screening? Retrieved from https://book.health.gov.sg/healthiersg-screening
(4) National University Cancer Institute Singaporehttps://www.ncis.com.sg/cancer-information/screening-and-prevention/cervical-cancer
(5) WHO – GLOBOCAN 2022. South–Eastern Asia
(6) Hasenleithner, S.O. & Speicher, M.R. (2022). How to detect cancer early using cell-free DNA. Cancer Cell, 40(12), 1464–1466.
DOI: 10.1016/j.ccell.2022.11.009
(7) WHO, American Cancer Society 2024 and USPSTF recommendations
(8) Nguyen, et al., 2025. “Prospective validation study: a non-invasive circulating tumor DNA-based assay for simultaneous early detection of multiple cancers in asymptomatic adults.” BMC Medicine 23, 90. https://doi.org/10.1186/s12916-025-03929-y
(9) Le Son Tran et al. 2025. Multimodal analysis of cell-free DNA enhances differentiation of early-stage breast cancer from benign lesions and healthy individuals. BMC Biology. doi: 10.1186/s12915-025-02371-z
(10) Li, Z., & Sun, Y. (2024). Circulating tumor DNA methylation detection as biomarker and its application in tumor liquid biopsy. MedComm, 5(2), e337. https://doi.org/10.1002/mco2.337
(11) USPSTF. (2016). Lehman, et al. Radiology.
(12) Mann, R. M., Athanasiou, A., Baltzer, P. A. T., et al. “Breast cancer screening in women with extremely dense breasts: Recommendations of the European Society of Breast Imaging (EUSOBI).” European Radiology, 32, 4036–4045 (2022)
https://doi.org/10.1007/s00330-022-08617-6
(13) Zhang, Y., Rodriguez, J., Mao, X., et al. “Incidence and risk factors of interval and screen-detected breast cancer.” JAMA Oncology, 11(5), 519–527 (2025). https://doi.org/10.1001/jamaoncol.2025.0167
(14) Jain D, Sethi S. Optimal Strategies for Colorectal Cancer Screening. Curr Treat Options Oncol. 2022; 23:474–493. DOI: 10.1007/s11864-022-00962-4
(15) U.S. Preventive Services Task Force Recommendation for Colorectal Cancer Screening
(16) NCCN Guidelines for Patients Colorectal Cancer Screening, 2024
